By Mark S. Jones
Neurofeedback can be a powerful and effective form of treatment for many problems, if done correctly. Many neurofeedback practitioners use automated report generators to process quantitative electroencephalograms (QEEGs). These generators come in the form of software that the clinician uses in their office, or by online services that do automated processing. Unfortunately, no matter how sophisticated these programs may be, they cannot replace the trained eye of someone who first examines the raw EEG. Nor can they replace the diagnostic ability of a trained clinician to assess the client’s symptoms and develop a proper treatment plan to address those symptoms.
Let’s look at an example of an automated report of an adult who presented with obsessive-compulsive behaviors and anxiety. This person also complained of insomnia and various cognitive problems, such as attention and short-term memory. An EEG recording was done by another neurofeedback practitioner and processed through an automated report generator that is probably one of the most sophisticated generators on the market today. In general, this analysis shows problems typically found with these reports: (1) reference pollution, (2) artifact treated as brain wave activity, and (3) not identifying research-based markers for certain relevant symptoms. The results include misdiagnosis and incorrect treatment protocols. These issues underscore the need for training and skill in making psychological assessments, reading the EEG, and understanding the limitations of QEEG findings.
Reference pollution
The montage used to process the EEG was Linked Ears, where all scalp electrode signals are compared to electrodes placed on the ear lobes or mastoids. A significant percentage of people, however, have measureable brain wave activity at the ear lobes which often originates from the medial and posterior temporal lobes in the brain. If brain wave activity is present in the reference electrodes, then all of the scalp electrode channels are polluted with this signal and will likely give a false reading of the location of these signals. One tell-tale sign of reference pollution is the appearance of wave oscillations that peak simultaneously in all channels. Actual brain waves do not appear in this manner. See the shaded area in the tracings below and observe the larger wave forms (alpha) that all peak simultaneously. One result is that certain brain waves may look more widespread that they are.
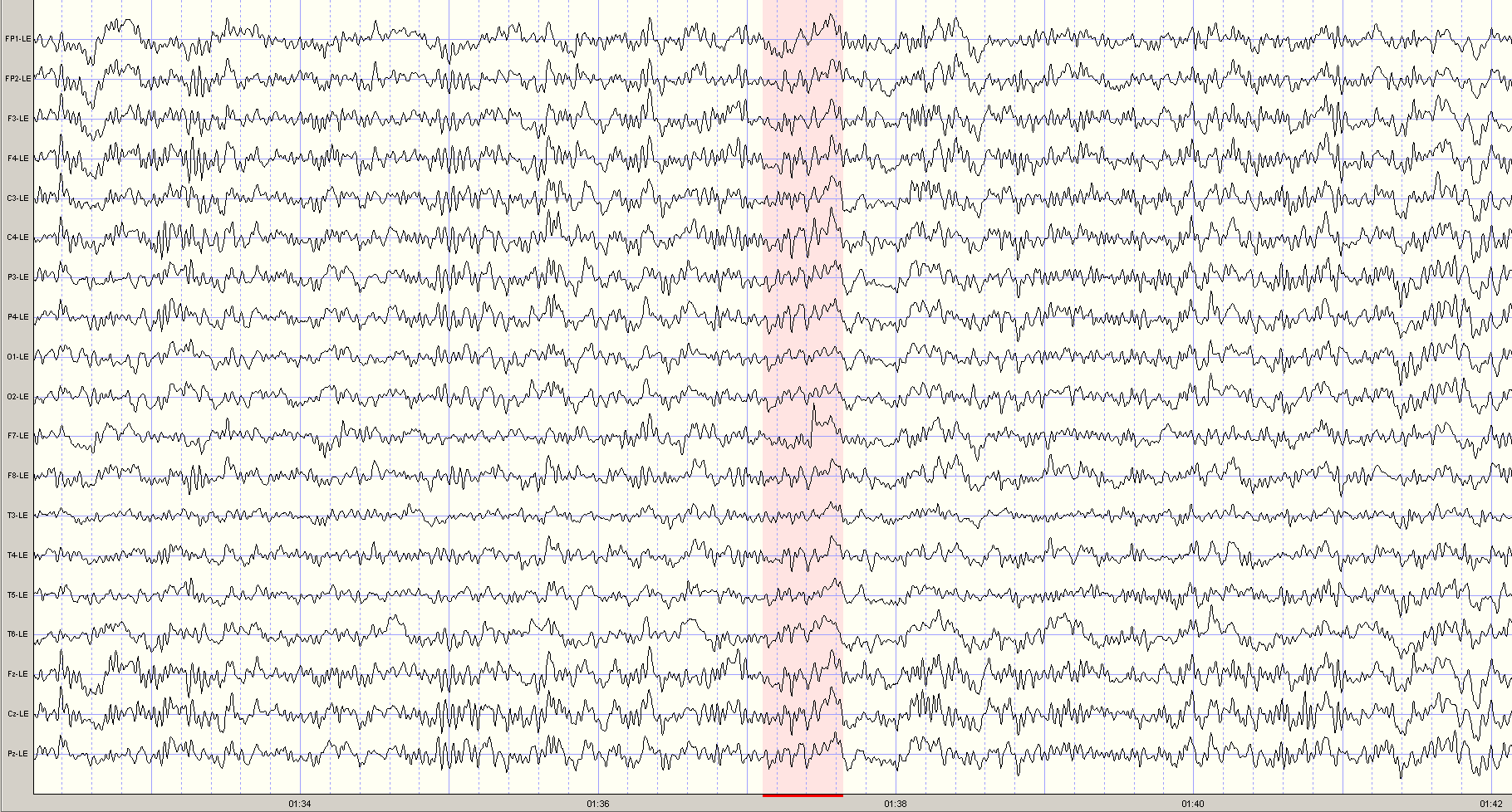
Automated report generators are simply not able to distinguish between reference pollution and actual brain waves patterns. The following excerpt is taken from an actual report produced by an automatic report generator, from the same section of the EEG recording.
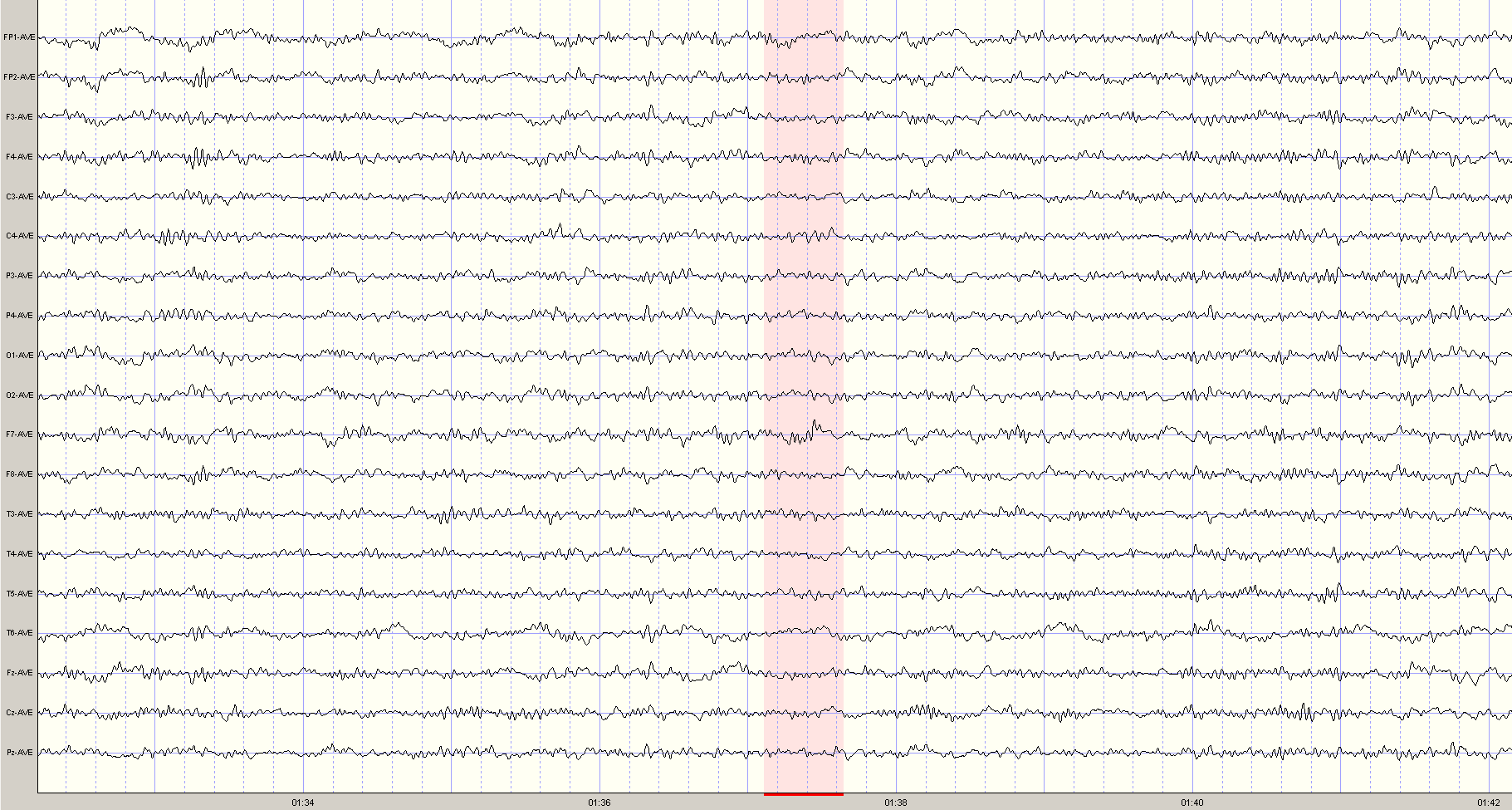
By using a different montage that does not use ear lobe references, a more accurate picture of true brain wave activity is revealed.
Artifact treated as brain activity
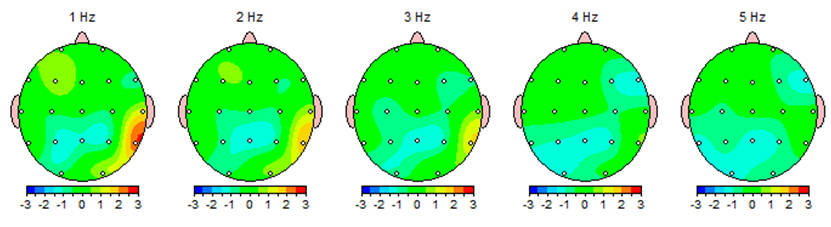
Artifact is any signal in the EEG that is not caused by brain activity, such as muscle tension, head movement, eye movement, swallowing, or heart beats. In this EEG, there is a distinct heart beat artifact in the T6 channel (above and behind the right ear). This particular artifact is referred to a cardio-ballistic or pulse artifact, and results from the expansion of a blood vessel due to heart beats which causes the effected electrode to move slightly and produces a slow up-and-down motion on the EEG tracing for that channel. See the example from this same segment of EEG:
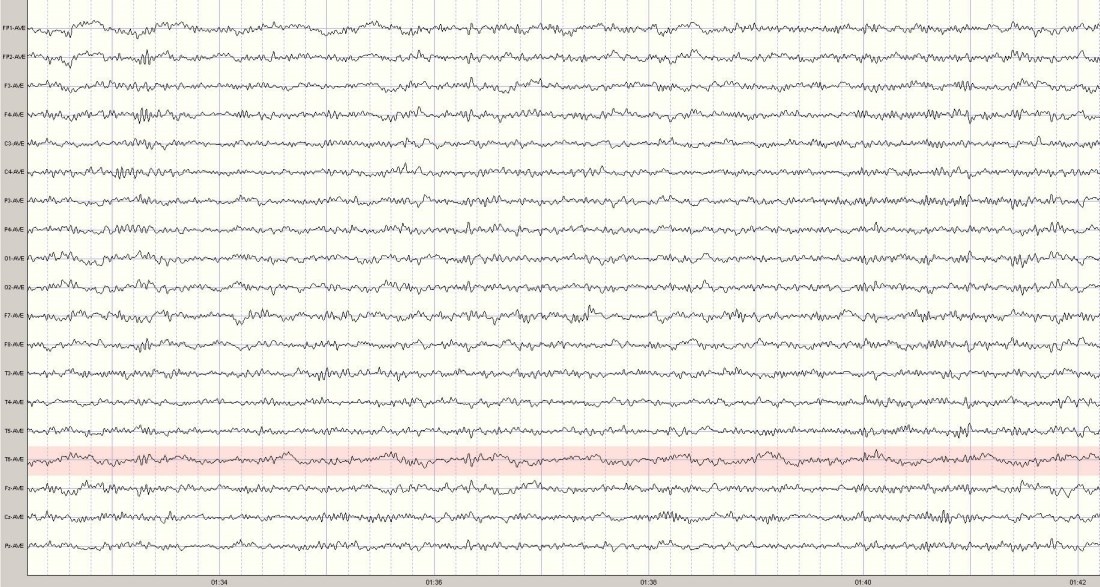
Unless this artifact is recognized by the clinician, it may well be mistaken as an abnormal brain wave and treated as such. In the automatic report generator, the artifact is visible in the topographic maps.
Unfortunately, the artifact also became a part of the treatment recommendations:
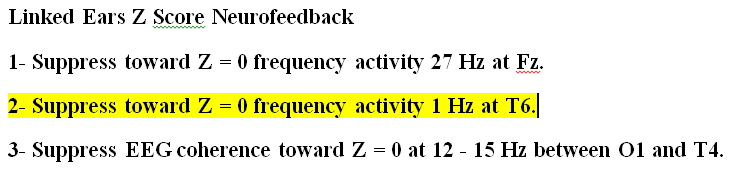
Does the clinician really want to attempt a protocol that is suppressing the client’s heart beat?
Additionally, it is also possible that the ear reference pollution distorted the coherence measures at T4, resulting in the questionable protocol (#3) above. Notice that the protocols are based on a linked ears montage, which in this case is polluted with artifact.
What is missing
A trained and experienced clinician would examine the EEG record and QEEG results to determine what brain wave abnormalities might be associated with the client’s symptoms. In this case there are two markers for anxiety and obsessive-compulsiveness: (1) beta spindles, and (2) attenuated alpha.
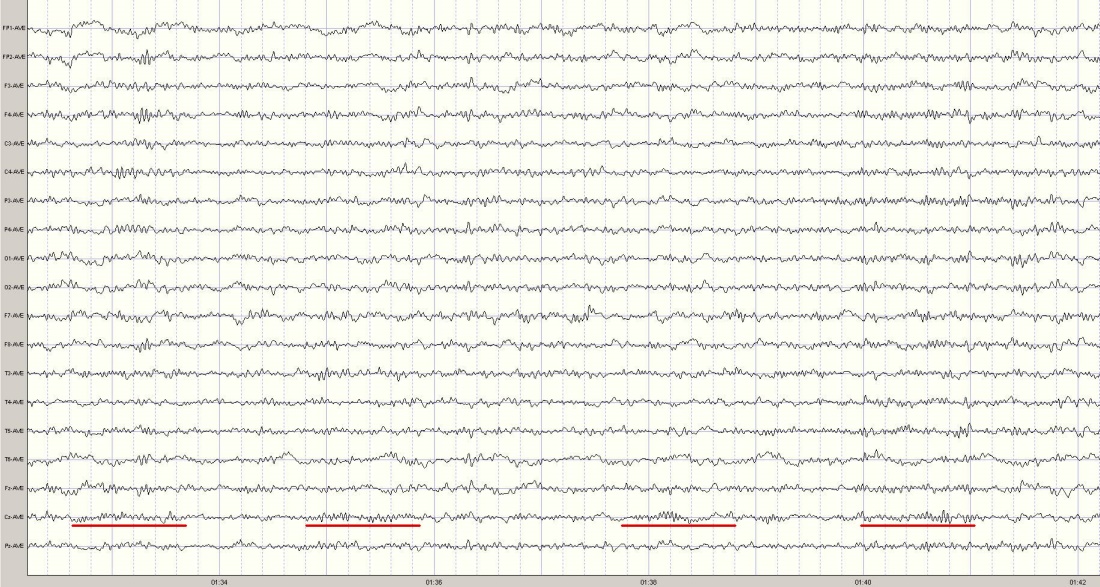
To the trained eye, the beta spindles are seen in the central region, centered at Cz. Examples are underlined in the EEG segment below.
This beta spindling activity is also depicted in the topographical maps and is most prominent at 27 cycles per second.
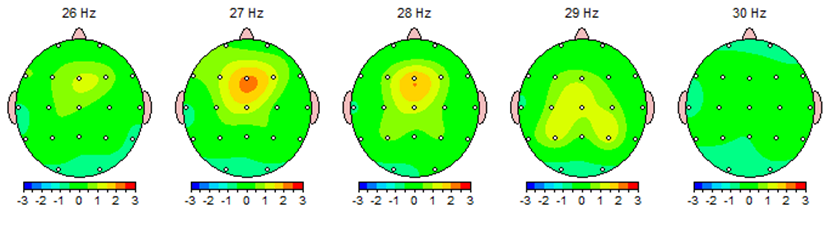
The shape of the waveform (spindling) reminded early electroencephalographers of a sewing spindle of thread. Automated report generators do not have the capacity to analyze brain waveforms (or morphology) for these types of research-supported biomarkers. The amplitude of this activity is statistically significant enough in this case to show up on the topographical maps and the protocol list, the treatment recommended is less than optimal. You will notice that the frequency of the waveform varies from 26-29hz. But, since only the 27hz activity exceeded the statistical model of the automated report generator, training was recommended only at that frequency, and would deny the client the benefit of training the entire frequency band of 26-28hz. Furthermore, while the amplitude of the waveform is highest at Fz, the tracings shown above show that the duration of the spindling activity is longest at Cz. Perhaps selecting a location between these two sites might be a better option.
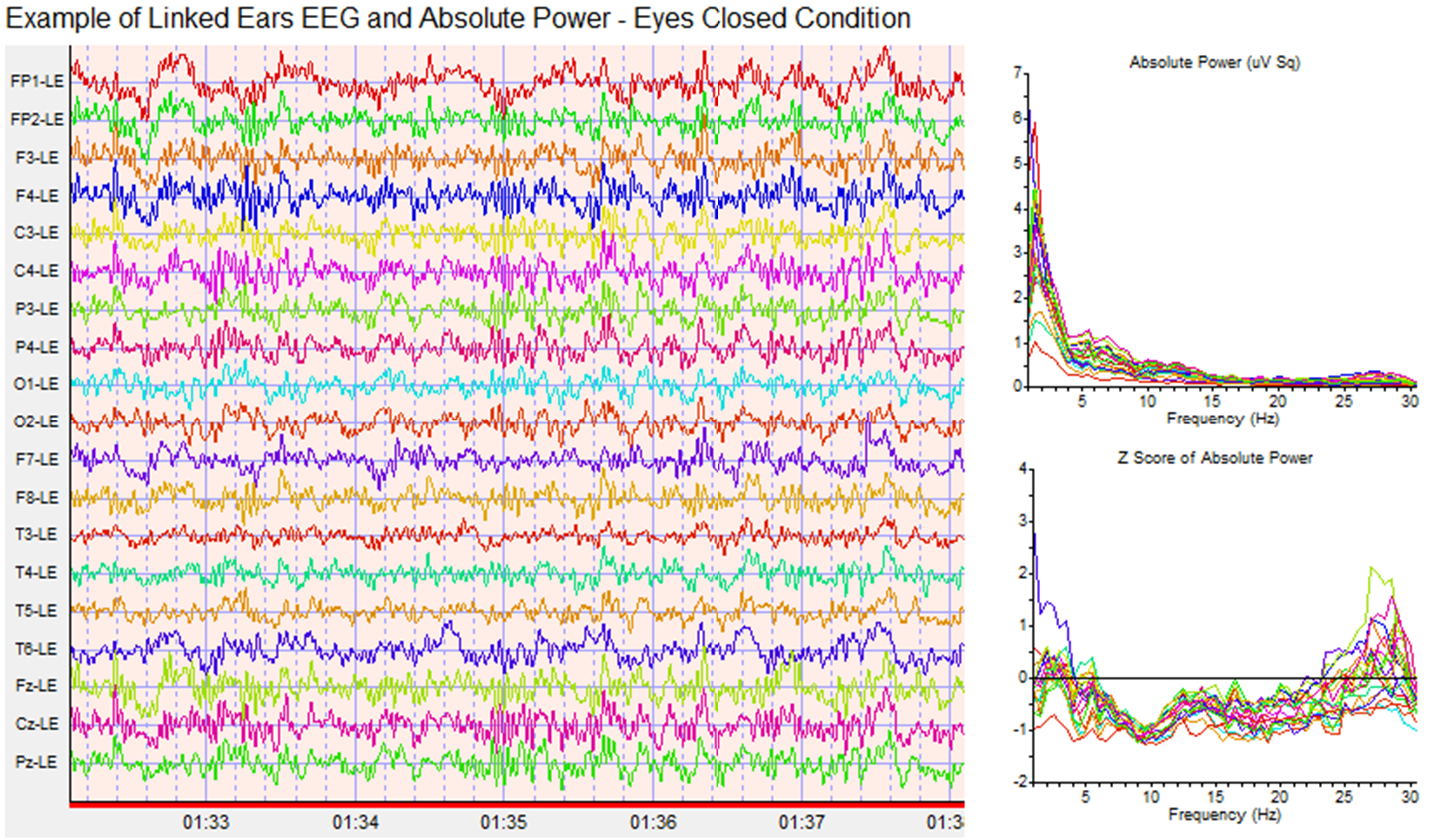
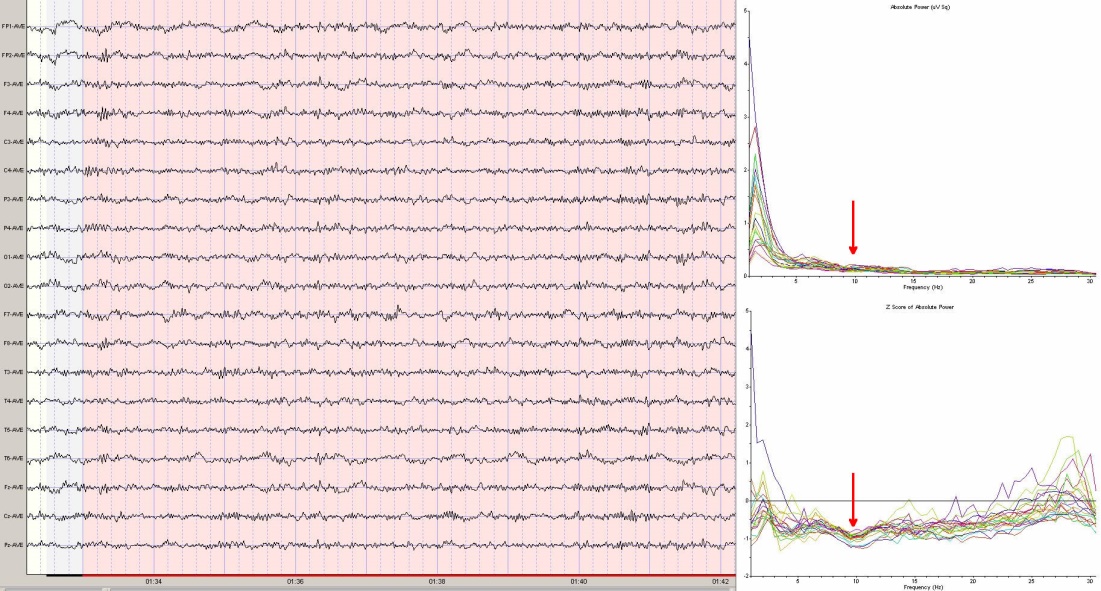
What is missing from the record is any organized, dominant alpha pattern—normally seen during an eyes closed recording. For adults, the alpha peak frequency is normally around 10hz. The following spectra graphs show where the alpha peak would be, if it were present. Additionally, the Z score (statistical) spectra graph shows a dip instead of a peak, further accentuating the absence of a normal alpha pattern.
Attenuated alpha has been shown to be associated with anxiety in some persons, and may be a marker for emotional trauma. However, the automated report fails to register this pattern. No protocol is recommended by the report for addressing this issue. Eyes closed, posterior alpha training has been found to be helpful for these individuals.
When taken as a whole, the spectra depicts an EEG that may be considered of low amplitude and fast in frequency, yet another marker for cortical overarousal, such as is often seen with persons who have anxiety and obsessive-compulsive tendencies. Since persons with these symptoms often complain of sleep and attention problems, it is likely that with improvement in the obsessive-compulsive and anxiety symptoms, the other issues would improve as well.